Find Your Solution
In 3 minutes, you’ll know where to start ➤
OCD Case Study: How a 7-Year-Old Misdiagnosed With Anxiety Finally Got the Right Help
This OCD case study follows Iris, a 7-year-old girl whose fears, rituals, and compulsive questioning had been growing for years — quietly labeled as anxiety, quietly getting worse.
Iris wasn't a child who appeared obviously unwell. She was shy, conscientious, and eager to please. But underneath that, her nervous system was running on overdrive — caught in a cycle of intrusive thoughts, reassurance-seeking rituals, and a brain that simply could not settle. And the people around her, including her therapists, had been accidentally making it worse.
By the time her parents found us, Iris had been in therapy for over a year, had a referral for psychiatric medication waiting, and was falling further behind every week. What she didn't have was the right diagnosis — or the right approach.
This is Iris's story — and a look at what becomes possible when a child's brain finally gets the calm it needs to do the hard work of healing.
Iris wasn't a child who appeared obviously unwell. She was shy, conscientious, and eager to please. But underneath that, her nervous system was running on overdrive — caught in a cycle of intrusive thoughts, reassurance-seeking rituals, and a brain that simply could not settle. And the people around her, including her therapists, had been accidentally making it worse.
By the time her parents found us, Iris had been in therapy for over a year, had a referral for psychiatric medication waiting, and was falling further behind every week. What she didn't have was the right diagnosis — or the right approach.
This is Iris's story — and a look at what becomes possible when a child's brain finally gets the calm it needs to do the hard work of healing.
Client Details

Iris (name changed to protect privacy)
Treatments

CALM PEMF®

Brain-based regulatory therapies

Nutrition and wellness coaching

Dietary Supplements

Gut support

Parent coaching (using the CALMS Dysregulation Protocol®)

Exposure and Response Prevention (ERP) therapy
Metrics

QEEG Brain Map (3)

Cognitive and Emotional Symptom Checklist

Physiological Symptom Checklist

Symptom Progress Tracking Likert Scale

Client and Parent Interviews

Lab work
Iris's Story: A Little Girl With Big Fears and a Brain That Couldn't Quiet Down
Iris is a 7-year-old girl with a history of anxiety and obsessive and compulsive behavior. Her story is one that many families will recognize — a child whose early signs were easy to explain away, whose distress grew slowly enough to normalize, and whose real diagnosis was hiding in plain sight for years.
A Difficult Start: Early Signs Nobody Named
Iris was born via cesarean section after her mother was in labor for more than twenty-four hours and signs of fetal distress were noted. Her Apgar score was initially five, improved to nine with oxygen, and she spent a few hours in the NICU as a precaution before being cleared.As a baby, she was difficult to settle — she needed constant holding and couldn't sleep on her own. Separation anxiety followed her all the way through preschool, requiring extended transition routines at drop-off and pickup. She was resistant to trying new things, and even when her siblings went first and showed her something was safe, Iris still needed coaxing.Looking back, these were the earliest signals of a nervous system that couldn't self-regulate. A child whose anxiety wasn't occasional — it was constant and structural.
The Question That Never Ended: Age Three and the Rise of Reassurance-Seeking
By age three, Iris had begun repeating questions she already knew the answers to. She needed reassurance — from her parents, her teachers, anyone nearby — delivered again and again before she could move forward. She knew the answer. That was never the point. The ritual of being told was what her nervous system was seeking.She transitioned to kindergarten with relatively few problems — her cousin was in her class, which smoothed the adjustment — and her teacher noted she was shy but completed her work. But the calm was fragile, and first grade shattered it.
First Grade: Perfectionism, Paralysis, and a System That Made Things Worse
First grade brought increased writing demands, and Iris's difficulties became impossible to manage quietly. Her anxiety and compulsive questioning intensified. Her perfectionism — her need for everything to be "just right" — began to prevent her from submitting work at all. The school responded by reducing her workload to relieve the pressure.It had the opposite effect. With fewer assignments, Iris simply devoted more time and energy to perfecting each one. The accommodation designed to help her was feeding the OCD cycle instead.This is one of the most important things I help families and schools understand: accommodating OCD — however kindly intended — makes it stronger. Every time we protect a child from the discomfort their fear produces, we confirm to their nervous system that the fear was worth having. The rituals grow. The demands escalate. The world shrinks.
Diagnosed Wrong: A Year of Missing the Right Treatment
Iris's parents sought therapy when she was six. She was diagnosed with generalized anxiety disorder and began working with a therapist who specialized in anxious children. The focus was on mindfulness-based stress reduction and helping Iris name her feelings. Iris got worse.They switched to a play-based therapist. Iris improved for a few months, then regressed again.The second therapist recommended a referral to a psychiatrist for an SSRI. Iris's parents researched the side effects and hesitated. And in that pause, they began to ask a different question: what if this wasn't anxiety disorder at all?Iris's aunt had OCD. The presentation wasn't identical — but the irrational, compulsive behaviors and obsessive thinking had the same texture. Her parents started to wonder if that was what they were actually looking at.
Finding the Right Map: A Brain Scan That Finally Explained Everything
Iris's parents found me through a Google search and read It's Gonna Be OK! before booking an intake appointment with a QEEG Brain Map. What the brain map showed was unambiguous: a pattern consistent with OCD — high Beta activity and overstimulated brain communication, one of the four common neurological signatures we see in children with OCD.The clinical picture was equally clear. Iris had specific, named fears: her parents and grandmother dying, her work being wrong, and that the kids at school didn't like her. Around each fear, she had developed rituals — ways of extracting reassurance from every adult in her life — and every adult, with the best intentions, had been complying. Parents, teachers, caregivers. Everyone was answering the questions. Everyone was providing the reassurance. Everyone was accidentally reinforcing the cycle.This is called a negative reinforcement loop — and it is one of the most common and most misunderstood drivers of OCD in children. The rituals weren't just habits. They were getting stronger every time someone gave Iris the reassurance she asked for, because each response confirmed that the fear had been worth expressing. The OCD was being trained, one answered question at a time.
A Difficult Start: Early Signs Nobody Named
Iris was born via cesarean section after her mother was in labor for more than twenty-four hours and signs of fetal distress were noted. Her Apgar score was initially five, improved to nine with oxygen, and she spent a few hours in the NICU as a precaution before being cleared.As a baby, she was difficult to settle — she needed constant holding and couldn't sleep on her own. Separation anxiety followed her all the way through preschool, requiring extended transition routines at drop-off and pickup. She was resistant to trying new things, and even when her siblings went first and showed her something was safe, Iris still needed coaxing.Looking back, these were the earliest signals of a nervous system that couldn't self-regulate. A child whose anxiety wasn't occasional — it was constant and structural.
The Question That Never Ended: Age Three and the Rise of Reassurance-Seeking
By age three, Iris had begun repeating questions she already knew the answers to. She needed reassurance — from her parents, her teachers, anyone nearby — delivered again and again before she could move forward. She knew the answer. That was never the point. The ritual of being told was what her nervous system was seeking.She transitioned to kindergarten with relatively few problems — her cousin was in her class, which smoothed the adjustment — and her teacher noted she was shy but completed her work. But the calm was fragile, and first grade shattered it.
First Grade: Perfectionism, Paralysis, and a System That Made Things Worse
First grade brought increased writing demands, and Iris's difficulties became impossible to manage quietly. Her anxiety and compulsive questioning intensified. Her perfectionism — her need for everything to be "just right" — began to prevent her from submitting work at all. The school responded by reducing her workload to relieve the pressure.It had the opposite effect. With fewer assignments, Iris simply devoted more time and energy to perfecting each one. The accommodation designed to help her was feeding the OCD cycle instead.This is one of the most important things I help families and schools understand: accommodating OCD — however kindly intended — makes it stronger. Every time we protect a child from the discomfort their fear produces, we confirm to their nervous system that the fear was worth having. The rituals grow. The demands escalate. The world shrinks.
Diagnosed Wrong: A Year of Missing the Right Treatment
Iris's parents sought therapy when she was six. She was diagnosed with generalized anxiety disorder and began working with a therapist who specialized in anxious children. The focus was on mindfulness-based stress reduction and helping Iris name her feelings. Iris got worse.They switched to a play-based therapist. Iris improved for a few months, then regressed again.The second therapist recommended a referral to a psychiatrist for an SSRI. Iris's parents researched the side effects and hesitated. And in that pause, they began to ask a different question: what if this wasn't anxiety disorder at all?Iris's aunt had OCD. The presentation wasn't identical — but the irrational, compulsive behaviors and obsessive thinking had the same texture. Her parents started to wonder if that was what they were actually looking at.
Finding the Right Map: A Brain Scan That Finally Explained Everything
Iris's parents found me through a Google search and read It's Gonna Be OK! before booking an intake appointment with a QEEG Brain Map. What the brain map showed was unambiguous: a pattern consistent with OCD — high Beta activity and overstimulated brain communication, one of the four common neurological signatures we see in children with OCD.The clinical picture was equally clear. Iris had specific, named fears: her parents and grandmother dying, her work being wrong, and that the kids at school didn't like her. Around each fear, she had developed rituals — ways of extracting reassurance from every adult in her life — and every adult, with the best intentions, had been complying. Parents, teachers, caregivers. Everyone was answering the questions. Everyone was providing the reassurance. Everyone was accidentally reinforcing the cycle.This is called a negative reinforcement loop — and it is one of the most common and most misunderstood drivers of OCD in children. The rituals weren't just habits. They were getting stronger every time someone gave Iris the reassurance she asked for, because each response confirmed that the fear had been worth expressing. The OCD was being trained, one answered question at a time.
Phase One: Cool the Brain on Fire — Before the Therapy Can Work
Iris's QEEG showed a brain that was over-activated and overstimulated. Before ERP therapy could be introduced — before Iris could be asked to tolerate the discomfort of resisting her compulsions — her nervous system needed to be calmed.
True to the Regulation First® principle, phase one focused entirely on reducing that overactivity: CALM PEMF® sessions, brain-based regulatory therapies, targeted dietary changes, supplements, and gut support. Parent coaching began immediately — not to change Iris's behavior directly, but to stop the inadvertent reinforcement that had been fueling the cycle. Every adult in Iris's life needed to understand what they were doing and why it needed to change.
Once Iris's brain began to settle, ERP therapy was carefully introduced.
True to the Regulation First® principle, phase one focused entirely on reducing that overactivity: CALM PEMF® sessions, brain-based regulatory therapies, targeted dietary changes, supplements, and gut support. Parent coaching began immediately — not to change Iris's behavior directly, but to stop the inadvertent reinforcement that had been fueling the cycle. Every adult in Iris's life needed to understand what they were doing and why it needed to change.
Once Iris's brain began to settle, ERP therapy was carefully introduced.
Phase Two: Teaching Iris to Talk Back to Her OCD
ERP — Exposure and Response Prevention — is the gold-standard treatment for OCD. It works by gradually exposing a child to the thoughts and situations that trigger their fears, while preventing the compulsive response that would ordinarily follow. Done well, it teaches the nervous system that the feared outcome doesn't actually happen — and that the anxiety, if not acted on, passes on its own.
But ERP only works when the brain is regulated enough to tolerate the process. Iris was initially resistant to even the smallest exposures. As her brain calmed through CALM PEMF® and supplements, her tolerance for the discomfort grew. The resistance softened. And then something remarkable happened — Iris began to enjoy it. She became proud of what she could do. She started bringing her wins to sessions.
Throughout this phase, the CALMS Dysregulation Protocol® guided the family's approach — giving Iris's parents a structured, science-backed framework for responding to the moments of dysregulation that still arose, without accidentally feeding the OCD cycle they were working so hard to break.
But ERP only works when the brain is regulated enough to tolerate the process. Iris was initially resistant to even the smallest exposures. As her brain calmed through CALM PEMF® and supplements, her tolerance for the discomfort grew. The resistance softened. And then something remarkable happened — Iris began to enjoy it. She became proud of what she could do. She started bringing her wins to sessions.
Throughout this phase, the CALMS Dysregulation Protocol® guided the family's approach — giving Iris's parents a structured, science-backed framework for responding to the moments of dysregulation that still arose, without accidentally feeding the OCD cycle they were working so hard to break.
As Iris's intrusive thoughts normalized and her anxiety reduced, she became noticeably more talkative, more social, and more open to the parent coaching that helped build her stress tolerance and coping skills.
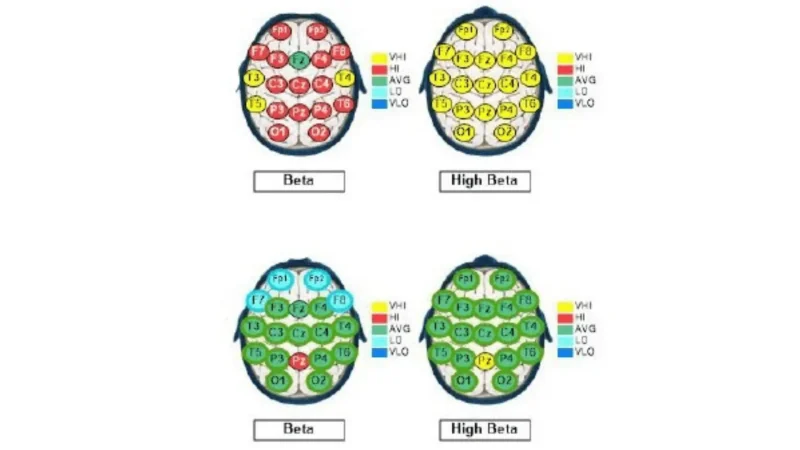
Before and After: QEEG Brain Map Comparison
The QEEG comparison — from Brain Map #1 to Brain Map #3 — shows the measurable neurological changes that took place over the course of treatment.
[Brain Map comparison image — QEEG #1 vs. QEEG #3 after 34 sessions of brain-based therapy, daily CALM PEMF®, and ERP psychotherapy]
[Brain Map comparison image — QEEG #1 vs. QEEG #3 after 34 sessions of brain-based therapy, daily CALM PEMF®, and ERP psychotherapy]
OCD Case Study Outcomes
After 34 sessions of brain-based therapy combined with daily CALM PEMF® via a mobile unit and ERP psychotherapy, Iris's overactive brainwave activity was reduced by more than 55%.
These weren't behavioral adjustments achieved through pressure or reward. They were the natural result of a regulated nervous system — exactly what the Regulation First® approach predicts and produces.

What This OCD Case Study Teaches Us
Iris's case carries lessons that are essential for any family navigating a child with anxiety-like symptoms that don't seem to be getting better:OCD is frequently misdiagnosed as anxiety — and the difference matters enormously. Anxiety and OCD overlap in how they look, but they respond to fundamentally different interventions. Mindfulness and reassurance-based approaches can actually worsen OCD by reinforcing the rituals that maintain it. Getting the right diagnosis isn't a formality. It changes everything about how you help.
Accommodating OCD makes it stronger. Every adult who answered Iris's repeated questions — however kindly — was reinforcing her nervous system's belief that the fear was real and the ritual was necessary. Understanding and interrupting this cycle was as important as anything we did clinically with Iris herself.
The brain must be calmed before ERP can work. ERP is the gold-standard treatment for OCD — but it requires a regulated nervous system to tolerate. Iris couldn't access the process until CALM PEMF® and brain-based therapy had reduced her overactivation enough to make the discomfort of exposure manageable.
Regulation First® is a sequence, not just a philosophy. Regulate. Connect. Correct. In that order, every time. When Iris's brain was calmer, the therapy reached her. The ERP worked. And the pride she felt in her own progress became its own form of healing.
Parent involvement changes the outcome. The CALMS Dysregulation Protocol® gave Iris's parents the tools to stop feeding the OCD cycle and start supporting her regulation instead. That shift — in how the adults around her responded — was as clinically significant as any intervention with Iris directly.
Accommodating OCD makes it stronger. Every adult who answered Iris's repeated questions — however kindly — was reinforcing her nervous system's belief that the fear was real and the ritual was necessary. Understanding and interrupting this cycle was as important as anything we did clinically with Iris herself.
The brain must be calmed before ERP can work. ERP is the gold-standard treatment for OCD — but it requires a regulated nervous system to tolerate. Iris couldn't access the process until CALM PEMF® and brain-based therapy had reduced her overactivation enough to make the discomfort of exposure manageable.
Regulation First® is a sequence, not just a philosophy. Regulate. Connect. Correct. In that order, every time. When Iris's brain was calmer, the therapy reached her. The ERP worked. And the pride she felt in her own progress became its own form of healing.
Parent involvement changes the outcome. The CALMS Dysregulation Protocol® gave Iris's parents the tools to stop feeding the OCD cycle and start supporting her regulation instead. That shift — in how the adults around her responded — was as clinically significant as any intervention with Iris directly.
A Note on Privacy
The names and some identifying details in this OCD case study have been changed to protect client privacy. Each client's experience and treatment protocol is unique and individually tailored based on their specific clinical profile.
Frequently Asked Questions About OCD Treatment in Children
Can I work with Dr. Roseann one on one?
I'm not taking individual clients right now, but that doesn't mean we can't work together! Through my Parent Certification Program, I teach you the exact tools and strategies I use in my practice — including the CALMS Dysregulation Protocol® — so you can apply them with your child at home. So many parents have told me it was the turning point for their family. [Learn more about the Parent Certification Program →]
What is the Regulation First® approach to OCD?
Regulation First® means we calm the nervous system before we ask it to do hard things — like tolerating the discomfort of ERP. Most OCD treatment jumps straight to exposure work, but a brain that's overactivated and on fire simply can't access that process. When we calm the brain first, the therapy works faster and the child stays engaged instead of shutting down.
What is the CALMS Dysregulation Protocol®?
The CALMS Dysregulation Protocol® is a five-step framework I developed to help parents respond to their child's dysregulation in a way that supports the nervous system rather than escalating it. It stands for: Co-regulate first, Avoid personalizing, Look for root causes, Model coping strategies, and Support and reinforce. For OCD specifically, it also helps parents stop the inadvertent reassurance-giving that feeds the OCD cycle — which is one of the most important things a family can change.
How do I know if my child has OCD and not anxiety?
This is one of the most common questions I hear, and it's such an important one. The key difference is the presence of rituals — compulsive behaviors that a child performs to reduce the anxiety produced by an intrusive thought. If your child is repeating questions they know the answers to, checking things repeatedly, needing things to be "just right," or performing routines that must happen in a specific way, those are OCD flags — not just anxiety. A QEEG Brain Map gives us objective neurological data that, combined with a thorough clinical intake, makes the distinction much clearer.
How long does it take to see results with OCD treatment?
It depends on how long the OCD has been active and how entrenched the rituals have become. What I can tell you is that when we calm the brain first and the family is fully on board, things move faster than most people expect. With Iris, the shift from resistant to engaged — and then to genuinely proud of her progress — happened over the course of treatment. The brain responds when you give it what it actually needs.
I'm not taking individual clients right now, but that doesn't mean we can't work together! Through my Parent Certification Program, I teach you the exact tools and strategies I use in my practice — including the CALMS Dysregulation Protocol® — so you can apply them with your child at home. So many parents have told me it was the turning point for their family. [Learn more about the Parent Certification Program →]
What is the Regulation First® approach to OCD?
Regulation First® means we calm the nervous system before we ask it to do hard things — like tolerating the discomfort of ERP. Most OCD treatment jumps straight to exposure work, but a brain that's overactivated and on fire simply can't access that process. When we calm the brain first, the therapy works faster and the child stays engaged instead of shutting down.
What is the CALMS Dysregulation Protocol®?
The CALMS Dysregulation Protocol® is a five-step framework I developed to help parents respond to their child's dysregulation in a way that supports the nervous system rather than escalating it. It stands for: Co-regulate first, Avoid personalizing, Look for root causes, Model coping strategies, and Support and reinforce. For OCD specifically, it also helps parents stop the inadvertent reassurance-giving that feeds the OCD cycle — which is one of the most important things a family can change.
How do I know if my child has OCD and not anxiety?
This is one of the most common questions I hear, and it's such an important one. The key difference is the presence of rituals — compulsive behaviors that a child performs to reduce the anxiety produced by an intrusive thought. If your child is repeating questions they know the answers to, checking things repeatedly, needing things to be "just right," or performing routines that must happen in a specific way, those are OCD flags — not just anxiety. A QEEG Brain Map gives us objective neurological data that, combined with a thorough clinical intake, makes the distinction much clearer.
How long does it take to see results with OCD treatment?
It depends on how long the OCD has been active and how entrenched the rituals have become. What I can tell you is that when we calm the brain first and the family is fully on board, things move faster than most people expect. With Iris, the shift from resistant to engaged — and then to genuinely proud of her progress — happened over the course of treatment. The brain responds when you give it what it actually needs.
Ready to Find a Path Forward?
If Iris's story sounds like your child, you don't have to keep trying approaches that are missing the root cause.
[Learn More About How We Can Help →]
[Learn More About How We Can Help →]
The effectiveness of diagnosis and treatment varies by patient and condition. Dr. Roseann Capanna-Hodge, LLC does not guarantee specific results.




